Lysol is a disinfectant designed for use on surfaces and contains phenol, a protoplasmic poison. Poisoning from Lysol can occur through oral ingestion, skin contact, inhalation, and other means. Phenol is mainly metabolized by the kidneys, and after absorption, it causes widespread capillary damage and clotting in superficial blood vessels. This results in urine that is scanty with traces of albumin, and microscopically, blood and calcium oxalate crystals are observed. The urine turns olive green or brown on standing, a phenomenon called carboluria.Studies by J. Jyrkkanen 2020 on antibiotic impacts on mitochondria showed that ROS damage and ruptures of mitochondria resulted in pathology leading to loss of oxidative phosphorylation, likelihood of increase in cancers favorite metabolism aerobic glycolysis, suppression of the p53 DNA repair gene, cardiovascular ailments and immune dysfunction. The similarity of damage reported here by google AI suggest a similar pathology for Lysol type antibiotic cleaners.Otherwise damaged mitochondria induced effects have been observed also for some common pesticides, and mRNA vaccine.The problem arises from the fact that Lysol is an antibiotic that kills bacteria and mitochondria are a highly modified essential symbiotic derivative of an ancient bacteria.
Characteristics
Values
Sensation
Constriction around the throat, burning pain from the mouth to the epigastrium
Taste
Sour and acidic
Urine
Scanty, with traces of albumin
Microscopic Observations
Blood and calcium oxalate crystals
Other Observations
Burns on the face and skin, mucosa of the mouth, tongue, pharynx, and esophagus may be bleached
Phenol Metabolism
Converted into hydroquinone and pyrocatechol, then excreted in urine
Urine Color
Olive green or brown on standing (carboluria)
Impacts on Mitochondria
The active ingredient benzalkonium chloride reveal a pattern of cellular toxicity mediated by mitochondrial damage.
Disruption of Energy Production
QACs which are commonly used in antimicrobial products, have been shown to inhibit mitochondrial respiration specifically at Complex I of the electron transport chain, leading to a decrease in cellular energy (ATP)
Structural Damage or Fragmentation
Exposure to these compounds causes structural disruption, resulting in mitochondrial fragmentation and changes in mitochondrial membrane potential
Induction of Oxidative Stress
Similar to other chemical sanitizers, these compounds can induce the generation of reactive oxygen species (ROS) within the mitochondria, causing further impairment.
Initiation of Apoptosis
Mitochondrial dysfunction caused by these surfactants can trigger the mitochondrial pathway of apoptosis or programmed cell death
Compounds with Documented Mitochondrial Toxicity
Quaternary Ammonium Compounds (QAC’s/BAC’s) induce mitochondrial dysfunction in epithelial cells
Cetylpyridinium Chloride (CPC)CPC causes severe nanostructural disruption, reduces ATP production, and acts as a mitochondrial inhibitor.
Ammonium Hydroxide a caustic compound present in some cleaners can cause severe irritation and potential cellular disruption.
CONCLUSION
These disinfectants can cause significant mitochondrial dysfunction in mammalian cells leading to significant morbidity and mortality. While disinfectant effect may reduce exposure to pathogenic microbes in the short term the harm to beneficial endogenous mitochondria may cause health issues in the long term.
References
Jyrkkanen jccm-aid1104
Jyrkkanen J. Antibiotic induced changes to mitochondria result in potential contributions to carcinogenesis, heart pathologies, other medical conditions and ecosystem risks. J Cardiol Cardiovasc Med. 2020; 5: 163-171
I chose a small sample of 1988 Agriculture Canada Inerts from a thick stack provided by MP Jim Fulton to run an AI search of toxicology and found significant toxicity and lethal potential including acute and chronic and epigenetic potential to cause death and serious health issues hidden behind a smokescreen of the word INERTS.
Alkyl benzene sulfonate… Inhalation tox, fish tox, microbial tox
Aloe extract….P 2B Human Carcinogen
Aromatic Hydrocarbon…Carcinogen, DNA damage, cardiovascular tox, immune dysfunction, pneumonitis
Asbestos fiber…Mesothelioma, Inflammation, Ovarian Cancer
ATLOX…Tox varies w brand
Benzene…Leukemogen
Ca(CN)2 Highly toxic lethal blocks cytochrome C oxidase in mitochondria
LINKS BETWEEN RF AND EMF AND BRAIN CANCERS. JORMA JYRKKANEN RESEARCHER 2025-03-25
Key Points
Research suggests a possible link between long-term exposure to electromagnetic fields (EMF) and radiofrequency (RF) radiation from cell towers and increased risk of brain cancers and Schwannomas, but evidence is not conclusive.
The International Agency for Research on Cancer (IARC) classifies RF radiation as “possibly carcinogenic to humans,” highlighting ongoing controversy.
Studies show mixed results, with some finding small increases in certain tumors, especially in animal studies, while human studies often show no clear association.
Avoidance guidelines include reducing call time, using speaker mode or headphones, and maintaining distance from cell towers, though effectiveness varies.
Overview
The connection between EMF, RF, and cell tower frequencies and brain cancers like gliomas and Schwannomas (tumors of nerve cells, including acoustic neuromas) is a complex and debated topic. While some studies suggest potential risks, especially with long-term exposure, the evidence is not definitive, and expert opinions differ.
Current Research Findings
Research leans toward a possible association, particularly with heavy, long-term use of cell phones and proximity to cell towers. For instance, the National Cancer Institute (NCI) notes stable brain tumor rates despite increased cell phone use, but animal studies, like those by the National Toxicology Program (NTP), found small increases in heart Schwannomas in male rats exposed to RF radiation (Cell Phones and Cancer Risk Fact Sheet – NCI). The IARC’s 2011 classification of RF as “possibly carcinogenic” reflects limited evidence, fueling ongoing debate.
Types of Cancers and Tumors
Brain cancers, such as gliomas, and Schwannomas, particularly acoustic neuromas, are of concern. Some studies, like the Interphone study, found a small increase in glioma risk for heavy cell phone users, while others, like the Danish Cohort, found no association. Schwannomas, linked to nerve cells, showed increased risk in animal studies but inconsistent results in humans.
Avoidance Guidelines
To minimize exposure, experts suggest reducing call duration, using speaker mode or wired headphones, avoiding calls in areas with weak signals (which increase emission), and maintaining distance from cell towers. The Food and Drug Administration (FDA) recommends these measures, though their impact on reducing cancer risk is not fully proven (Reducing Radio Frequency Exposure from Cell Phones – FDA).
Survey Note: Detailed Analysis of EMF, RF, and Cell Tower Frequencies Linked to Brain Cancers and Schwannomas, Including Avoidance Guidelines
This note provides a comprehensive overview of the relationship between electromagnetic fields (EMF), radiofrequency (RF) radiation, and cell tower frequencies with brain cancers and Schwannomas, including detailed findings from recent studies and practical avoidance guidelines. The analysis is grounded in current scientific literature, with a focus on clarity for a lay audience while maintaining technical accuracy.
Introduction
EMF and RF radiation are forms of non-ionizing electromagnetic radiation emitted by cell towers, cell phones, and other wireless devices. Cell towers operate at frequencies typically ranging from 700 MHz to 2.7 GHz for 2G, 3G, and 4G, and up to 80 GHz for 5G, as noted by the NCI (Cell Phones and Cancer Risk Fact Sheet – NCI). Concerns arise about potential links to brain cancers (e.g., gliomas, meningiomas) and Schwannomas, which are tumors of Schwann cells, often manifesting as acoustic neuromas. This note synthesizes findings from epidemiological, animal, and expert reviews, acknowledging the complexity and controversy surrounding the topic.
Scientific Evidence and Findings
Epidemiological Studies in Humans
Human studies provide mixed results, with no definitive link established. The NCI’s fact sheet, updated in April 2024, indicates stable incidence rates for adult gliomas, pediatric brain tumors, and acoustic neuromas in the US and other regions, despite increased cell phone use (Cell Phones and Cancer Risk Fact Sheet – NCI). Key studies include:
Danish Cohort Study: No association with glioma, meningioma, or acoustic neuroma, even for subscribers over 13 years, with ORs not significantly elevated (Cell Phones and Cancer Risk Fact Sheet – NCI).
Million Women Study: No association with glioma, meningioma, or non-CNS tumors; initial acoustic neuroma association was not sustained with longer follow-up (Cell Phones and Cancer Risk Fact Sheet – NCI).
COSMOS Study: Among 264,574 participants, no association with glioma, meningioma, or acoustic neuroma, with median follow-up over 7 years (Cell Phones and Cancer Risk Fact Sheet – NCI).
CERENAT (France): No association for regular users, but heaviest users showed increased glioma and meningioma risks, suggesting a dose-response relationship (Cell Phones and Cancer Risk Fact Sheet – NCI).
Swedish Pooled Analysis: Found increased brain cancer risk for use before age 20, an unexpected detail given children’s theoretical vulnerability due to developing nervous systems (Cell Phones and Cancer Risk Fact Sheet – NCI).
Children’s Studies (CEFALO, MOBI-Kids): No increased cancer risk in children aged 7–19 and 10–24, respectively, despite theoretical concerns (Cell Phones and Cancer Risk Fact Sheet – NCI).
Animal Studies
Animal studies provide some evidence of potential risks, particularly for Schwannomas. The NTP and Ramazzini Institute found small increases in heart Schwannomas in male rats exposed to RF radiation at 3, 6, or 9 watts per kilogram for 18 hours daily, but these findings are limited by species differences and rarity in humans. The NCI notes these results raise questions but do not conclusively link to human brain cancers (Cell Phones and Cancer Risk Fact Sheet – NCI). Another study on 1800 MHz RF-EMF exposure showed inhibited neurite outgrowth in embryonic neural stem cells at 4 W/kg for 3 days, suggesting potential developmental impacts (Exposure to 1800 MHz radiofrequency radiation impairs neurite outgrowth of embryonic neural stem cells | Scientific Reports).
Occupational and Environmental Exposures
For workers with high RF exposure, such as Navy electronics technicians, some studies suggest increased risks of non-lymphocytic leukemia and brain cancer, but results are inconsistent. The NCI’s fact sheet on EMF and cancer notes early studies (1980s–1990s) reported higher cancer rates in electrical occupations, but recent studies with exposure measurements generally show no increased risk (Electromagnetic Fields and Cancer – NCI). Children living near power lines with exposures ≥0.3–0.4 μT showed a 1.4–1.7-fold increased risk of leukemia in pooled analyses, affecting a small percentage (<3%) of children, but mechanisms remain unclear (Electromagnetic Fields and Cancer – NCI).
Expert Opinions and Classifications
The IARC classified RF radiation as “possibly carcinogenic to humans” (Group 2B) in 2011, based on limited evidence from human and animal studies, reflecting ongoing controversy (Cell Phones and Cancer Risk Fact Sheet – NCI). The American Cancer Society, NIEHS, FDA, CDC, FCC, and European Commission (2015) generally conclude no definitive evidence of harm, with calls for more research. The European Commission found no increased brain tumor risk from RF exposure but noted an open question for acoustic neuroma (Electromagnetic Fields and Cancer – NCI).
Frequency Bands and Exposure Levels
Cell towers emit RF in bands like 850 MHz, 1900 MHz, and higher for 5G, with exposure measured by Specific Absorption Rate (SAR), typically below 0.1 W/kg in studies, far below thermal effect thresholds. The FCC provides SAR data for devices, and the NCI notes exposures are generally within safety limits (Cell Phones and Cancer Risk Fact Sheet – NCI).
Avoidance Guidelines
Given the uncertainty, several practical measures can reduce exposure, though their effectiveness in preventing cancer is not proven:
Reduce Call Time: Limit duration of calls, especially long conversations.
Use Speaker Mode or Headphones: Use wired headphones or speaker mode to increase distance from the head.
Avoid Calls in Weak Signal Areas: Weak signals increase emission power, so prefer texting or waiting for stronger signals.
Maintain Distance from Cell Towers: Avoid prolonged proximity to cell towers, though residential exposure is typically low.
The evidence suggests a possible link between long-term EMF/RF exposure and brain cancers/Schwannomas, but it is not conclusive, with significant controversy. Human studies often show no clear association, while animal studies and some occupational data raise concerns. This may be due to differential synergist like viral exposures exposure histories alone [J. Jyrkkanen 2025, comm.]. Avoidance guidelines offer precautionary measures, though their impact on cancer risk reduction is uncertain. Given the 2025 context, ongoing research, such as the COSMOS study, continues to monitor long-term effects, emphasizing the need for balanced public health approaches.
Note self assembly of complex structures with blood clotting potential.
Toxicology
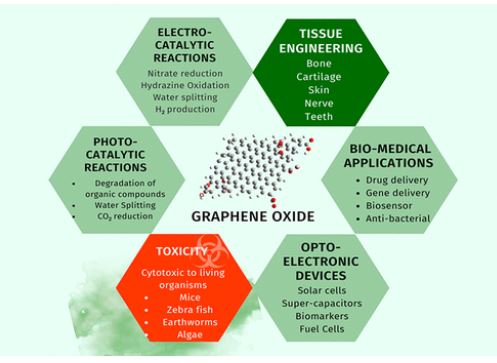
One feature that needs more attention is toxicity; it was discovered that the concentration of GO affects whether or not it is physiologically harmful, which restricts its use in the field of medicine. It has been found that there are a lot of animal species for which GO showed some cytotoxic nature.
Considerations
Note cytotoxic to living organisms like mice, zebra fish, earthworms, algae.
WATCH: A robot made of magnetic slime inside your body. GRAPHENE, COVID VAX Nanoparticles, technology used to create robots inside your body. They can kill or cause disease at will.
The slime, which can be controlled by a magnetic field, can move in confined spaces and grasp… pic.twitter.com/MHwO9DuPLx
My Lifetime Research Findings:After reading the following and following the links if you want further reading of my literature, try using these search terms after my name: Jorma Jyrkkanen antibiotics, cancer, oncology, cardiology, epigenetics, music, Jormawankenobe, birds, hiking, climate, virology, covid, spike, BWC, geopolitics, WEF, bombing, Deep State, evolution, Darwin, spallation, methylation, bald eagles, Khutzeymateen, Kvenland, extinction, Skagit, Books, blogspot.com, twitter, wordpress.com and follow the links. You may also explore my Bibliography which I add to on occasion. https://jormajyrkkanen.ca/2024/02/14/jorma-antero-jyrkkanens-bibliography-2024-02-14/
3. Ontario Minnesota Pulp and Paper company were liquidating the Ontario boreal forests by fudging regeneration statistics. Chief Forester George Brown shut them down and made them agree to Boreal Forest Clear cut Guidelines and regeneration plans.
4. Vision herbicide, a glyphosate Monsanto product, had 350 ppm of carcinogenic 1,4-dioxane in it and its surfactant polyoxyethyleneamine POEA added to its carcinogenic risk. https://jorma-jyrkkanen.livejournal.com/184872.html
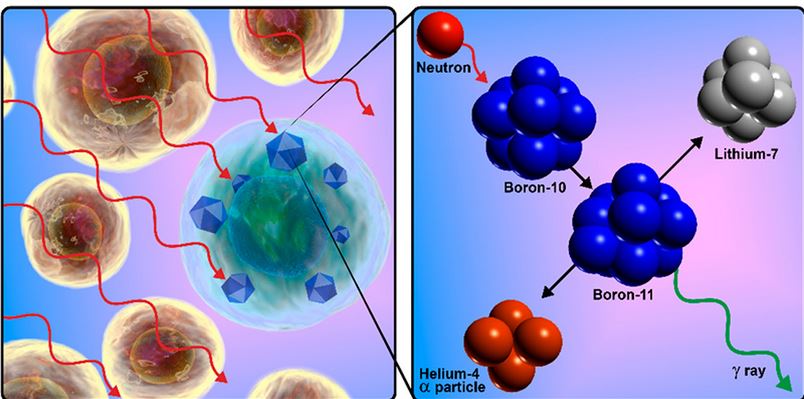
Spallation synthesis of Boron probably made life possible in the universe. It seems we owe our existence to high energy radiation as well as star stuff.
My Conclusion: Cosmic ray spallation is thought to be responsible for the abundance in the universe of some light elements—lithium, beryllium, and boron—as well as the isotope helium-3. They exist only by virtue of their nucleosynthesis during the Big Bang, and also cosmic ray spallation. These lighter elements in the present universe are therefore thought to have been produced through thousands of millions of years of cosmic ray (mostly high-energy proton) mediated breakup of heavier elements, spallation in interstellar gas and dust. This suggests life owes its existence much to spallation by proton radiation collaborating with star stuff.
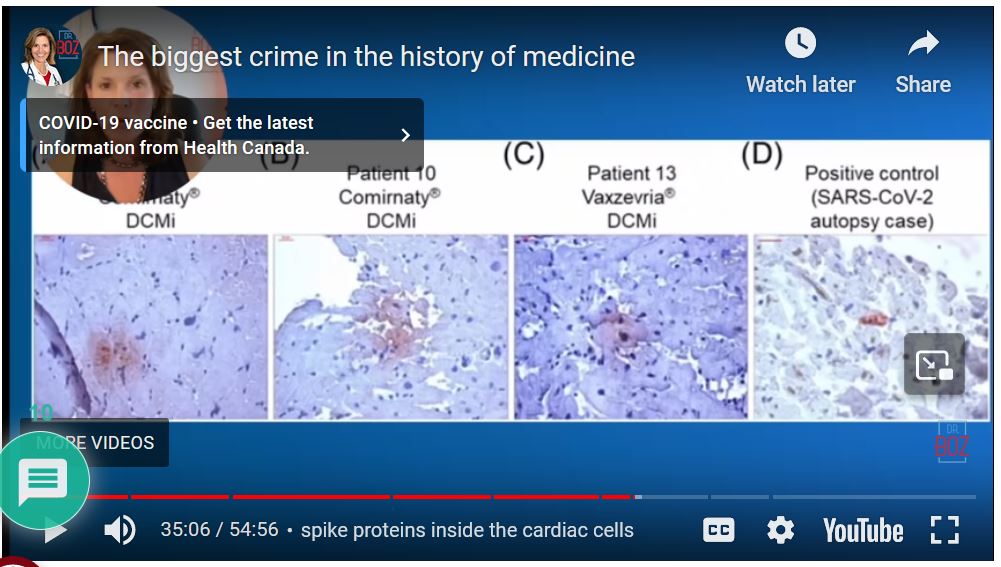
Pro-vaccination Dr blows whistle on vaccination and finds huge DNA contamination which can increase inflammation and myocarditis, SV40 linked to brain cancer, bone, NHL and malignant mesothelioma and spike protein in heart muscle on autopsy and batch switch from approved to mass produced for public use.
8. I gave evidence at in International Conference on Genetics, Genetic disorders and Stem Cells in Stockholm in 2018 that there is a pandemic of cancers caused by infectious agents ongoing and mouse mammary tumor virus (MMTV), simian virus 40 (SV40) needed to be added to the list of agents and Epstein Barr virus needs special attention. I computed a rough estimate of surplus cancer deaths worldwide attributable to infectious agents without considering gain-of-function bioweapons of approximately 2,365, 920 Deaths in 2023. This is now of course an under-estimate because we need to add the mortality from Turbo cancers from Covid-19 reported by Japanese, UK and American Oncologists. AIDS cancers ex: lung, anal, hepatocellular, Hodgkins lymphoma, oropharyngeal cancers, sars2 covid-19 cancers, SV40 cancers ex: SV40 may contribute to the development of mesotheliomas in humans. Epidemiological studies are needed. SV40, a monkey and now human polyomavirus, was introduced into the human population as a contaminant of vaccines. Merck Virologist Maurice Hilleman bragged about spreading SV40 tumors to Russian Olympians so America would win the Olympics.
I hereby declare that there is a global pandemic of cancers caused by infectious agents, most natural, some with possible increased pathogenicity by gain-of-function and enhanced transmissability (ex: HIV and SV40 by plandemic or injection). There is an increased risk of developing cancer from exposure to these pathogens and also transmit that risk to others by poor hygeine.
Microbiologist Kevin McKernan ran tests on covid vaccine approved and injected and found injected vaccine had DNA contamination and from sequence data was not the one that was approved.
Breaking News Pfizer Lawyer States We did no commit fraud, we delivered the Fraud the Government Ordered. Covid was a DOD fraud all along leading to over 17 Million Killed Worldwide.
Quoting Dr. David Martin: Peter Daszak wrote in 2015 ‘they needed the media to hype up the need for coronavirus vaccines to sell them’. The very next year Dr Ralf Baric wrote in 2016: ‘..’the (WIV) virus was human ready’ a clear indication a weapon was being readies for human transmission. [Seems to me J. Jyrkkanen ‘Collusion and Conspiracy to commit a bioweapon convention violation BWC for profit’]
21. How Prince Phillip, The Duke of Edinborough and I deliver the Khutzeymateen Grizzly Sanctuary to the World. I had to put this in because its such a good news story I was involved in.
For my conservation and habitat work I was given the honor of having a BC Park Named after me. I asked them to use my nic-name at work “FINN”. Ergo ‘FINN CREEK PARK’.
22. I computed the eigenvectors and principle eigenvalue of Squamish Wintering Bald Eagles to what I think is a close approximation from real data I happily gathered over four years and believe have nailed it. It tells me eagles have evolved a density dependent feedback system of population regulation that leads to growth and a stable age distribution. I Post it because its cool and used my UBC Zoology training beautifully. I think I deserve a PHd for this.
Computing Eigenvalues and Eigenvectors for Squamish River Wintering Bald Eagles. Jorma Jyrkkanen, jjyrkkanen76@outlook.com 3 Dec 2018 Background I fiddled with my 4 years of Squamish Wintering Eagles demographic data and fudged a bit of the model to add males in the Reproduction and got an interesting growth rate, lambda1 and a great Eigenvector or stable age distribution. Here it is. Will play with it until I am happy with data fit and may extend it out to 15-20 years age classes. It’s a dynamic model amenable to gaming based on thousands of field observations.
Discussion What I saw from year to year though were what looked like compensatory density dependent adjustments in age specific survival so it flip flopped p due to competition from yr to yr.
This fact is not amenable to deterministic Markov models like Leslie UNLESS you ‘game it’ or program in ‘if Sxi > or < Sxi critical-then-change-Sxi+ or-n’ ie compensatory survival feedbacks to other age classes. I urge population biology students to try it and watch amazing responses to population and age structure. I used an online Calculator bandicoot.maths.adelaide page written by Mathew Roughan.
Figure 1. Sample Leslie Matrix and Start Population Vector with test age specific reproductive rates for a Female Population based on Hypothetical Statistics to Observe Deterministic Model Responses in Total Population, Age Classes and Growth Rates (Primary Eigenvalue) and proportional age class structure (Eigenvectors).December 3, 2018Created by Jorma A. Jyrkkanen Note. The last three age classes are all adults and there is some presumption of productivity from four year class Bald Eagles ie R4=0.1
Eagles Run 2 with a Working Survivorship Population Vector but discrepancy in observed and model that works.
This latter run has a high crash potential (CP) in 8 yrs and a lot of fluctuation. For a more realistic model I have to incorporate my field data.
The bottom box has the stable age structure eigenvector and age specific eigenvalues. The latter more realistic run works but stability hangs on a few percentage survivorships of juveniles age classes and only includes 8 Age classes total.
Conclusion I concluded that the dynamic nature of feedbacks assures high survival of recruits to replace low adult mortality. Note how with even static Survivorships (Sij diagonals in L) there is an innate generation of wild fluctuations in age-class abundance in the curves at the bottom but I caution that in the field this is difficult to tease apart from random effects of migration linked as it is to weather and food availability. This phenomenon no doubt leads a lot of people to think a population is in trouble when only short-term observations are made and it is not true. Time lags are working to smooth out the age class distributions and real population. You only come to know these statistics as probably true after years of observation. I did 4 with thousands of observations and it was just starting to sink in. Keep in mind that these parameters apply only to the female side of the population. If you add the males it will approximately double.
I was a herd animal til I had a good look around. The Bulls liked the Lambs best.
FUNDING: I only received remuneration on discoveries 1 and 3. The remainder of all my scientific work and the thousands of hours I put in to them has been paid for by me and the hardship it imposed on my family. If some philanthropist has funds to chip in and reimburse me for my work for humanity and nature it would be helpful. My situation is very humble and I could do more with help. To help contact me by text message and we can talk on telegram.
I dedicate my life’s research to my Father and Mother who gave me life. Dad owed his life to a Railway spike. Attacked by Russians he ran out of bullets and a Soviet soldier came to shoot him but dad got him in the heart with a long thrown railway spike, took his firearm and continued the battle which the Finns won. None of my work would have happened without his strength and courage and a railway spike.
“The West wants war DESPERATELY with Russia. The Polish Foreign Minister Radoslaw Sikorski has come straight out and admitted on Friday, March 8th, that “NATO military personnel are already present in Ukraine.” They can’t wait to draw the first blood. Russia has NEVER had any intention of invading Europe. It has always been the other way around. This entire war was staged from the outset and was intended to force Russia to defend its own people in the Donbas. The West needs this war because the financial system can no longer be sustained. Governments default when they can no longer sell new debt to pay off the old. We are dangerously approaching that, and the war will be the excuse for default, like in World War II.
Danish Prime Minister Mette Frederiksen said she decided Denmark would send its artillery units to Ukraine. Meanwhile, NATO is moving nuclear missiles to the border with Russia. There is absolutely NOT ONE LEADER interested in seeking peace. Every single one is pushing for World War III ASAP. They all have their bunkers, so personally, they do not care about the people they are supposed to represent. The population has already been decided to be thinned out like a herd of sheep. Look at any war – more civilians ALWAYS die than soldiers.
There is no war where people have EVER been told the truth. Many in the so-called power positions were manipulated themselves. They are still debating the real causes behind World War I. I can tell you from what I know that the REAL reason behind the Iraq War was this idea of REGIME CHANGE throughout the Middle East would create peace by bringing in DEMOCRACY – which we do not even enjoy. Many officials do not know the real reason behind Iraq.
The object here has ALWAYS been Regime Change. These people convince themselves if they invade Russia and overthrow Putin, the Russian people will cheer. That is a bunch of Neocons patting each other on the bank as to how brilliant they are. The sanctions on Russia were supposed to get the stupid Russian people to rise up and overthrow Putin to remove the sanctions. I never heard such stupidity in my life. This is why NOT A SINGLE REASON for war ever involves the truth. They manipulate those in power, like hand-puppets, to do their bidding, as we see it taking place right now.
While the computer shows that Trump should win, I still cannot see how they will allow that to take place. They need Biden, and they are looking to start this war by May or July/August, JUST IN CASE Trump wins and their assassination schemes fail.”
Public Health Agency refusing to disclose uncensored documents on Winnipeg virus lab
Foreign affairs critic wants to know what Canada’s role was in training, equipping Wuhan virology lab
Karen Pauls · CBC News · Posted: May 11, 2021 2:40 PM PDT | Last Updated: May 11, 2021
Dr. Xiangguo Qiu at the at the National Microbiology Laboratory (NML) in Winnipeg. A special parliamentary committee on Canada-China relations wants to know why she and her husband were let go from the lab amid an RCMP investigation. (CBC)
As the Public Health Agency of Canada refuses to release uncensored internal documents, a Conservative MP says he wants to know how far Canada’s collaboration with China on Level-4 pathogens went — and why two federal scientists were let go by the National Microbiology Lab in Winnipeg in January.
“We need these documents. We need to know what the Government of Canada was doing through the National Microbiology Lab in Winnipeg with respect to cooperating with the Wuhan Institute of Virology in Wuhan, China,” Conservative foreign affairs critic Michael Chong said during a special parliamentary committee hearing on Canada-China relations Monday night.
The special committee has demanded to know why two federal government scientists were escorted out of Canada’s only Level 4 Lab in July 2019, just four months after one of them shipped samples of the Ebola and Henipah viruses to the Wuhan Institute of Virology in China — stories first published by CBC News.
Henipah Virus, Bats Rodents, Other Mammals, Humans Highly Fatal.
[Jyrkkanen Comm 2023. This virus has the potential to be abused and made more potent with gain of function attributes for dispersion and person to person contagion as a biowarfare agent and to act as a vector for population decline by a malevolent state biowarfare agency and as a tool to implement the NWO and Great Reset the Group of 300 and WEF are trying to achieve.Combined with EBola it would have enormous lethality.]
Two months after that shipment, on May 24, 2019, the Public Health Agency of Canada (PHAC) referred an “administrative matter” to RCMP that resulted in the removal of two Chinese research scientists — Xiangguo Qiu and her husband, Keding Cheng — and several international students on July 5.
Conservative MP Michael Chong says he wants to know why two scientists were let go from the National Microbiology Lab, why the RCMP is investigating them and whether the training the Winnipeg lab has given its counterpart in Wuhan, China has any connection with the origins of the COVID-19 pandemic. (Sean Kilpatrick/The Canadian Press)
The committee says it wants to know why Xiangguo Qiu and Keding Cheng were let go this past January.
“The Canadian public has the right to know what the extent of that cooperation was, why these two scientists there were terminated, and what exactly happened with the transfer of Henipah and Ebola viruses and any other workings and goings on between a Government of Canada institution and this virology lab in Wuhan,” Chong said.
Despite repeated requests from the committee, PHAC has refused to answer those questionsor provide uncensored internal documents, saying it can’t release personal information under federal privacy laws.
It did provide 271 pages of documents to the committee in advance of Monday’s meeting, but much of it was censored.
“We’ve redacted documents where the information pertains to personal information, investigations or security matters. The reason we’ve done so is that, as public servants, we’re bound by law to keep confidential information confidential,” PHAC president Iain Stewart told the committee.
“It’s not that we’re wishing to be uncooperative or unresponsive. We are disclosing as much as we can within the limits of the law.”
Iain Stewart, president of the Public Health Agency of Canada, says federal privacy law prevents him from sharing personal information about the two scientists let go from the National Microbiology Lab in Winnipeg. (National Research Council/Twitter)
Liberal MP Robert Oliphant, parliamentary secretary to the Minister of Foreign Affairs, told Stewart he should get a second opinion on that.
“I think the Justice Department is not giving you the best advice,” he said.
Stewart did provide more information on the shipment of Ebola and Henipah samples from Winnipeg to the Wuhan lab. He said the shipment was done properly.
“While this is the only time that we have shared virus samples with this particular lab, collaboration with labs outside of Canada are critical to advance public health research into infectious diseases,” he said.
“Given our standing as a collaborating partner for viral fever viruses, as well as our knowledge on regulations and standards for these types of transfers, the laboratory in Winnipeg is often asked to provide materials to new or existing programs, including laboratories in the United States.
“The [National Microbiology Lab] is open to providing materials in a safe, responsible and transparent fashion with other labs in order to foster global collaboration rather than enable research on any given disease to be monopolized by specific teams.”
Right to know
Conservative human rights critic Garnett Genuis said there is a precedent in a 2010 ruling for fulfilling the committee’s request for unredacted documents.
That ruling by the Speaker of the House of Commons found the Harper government breached parliamentary privilege when it refused to produce uncensored documents on the treatment of Afghan detainees. It ordered that the material be turned over to MPs.
Chong said Canadians have a right to know the full back story and the committee has the legal right to compel the release of unredacted documents.
He asked some pointed questions about what the National Microbiology Lab did to build up the capacity of its counterpart in Wuhan, China — a virology lab some have tried to link to the origins of the COVID-19 pandemic. Those theories have not been substantiated.
“There are two theories about how the coronavirus emerged. One is that it was zoonotic,” Chong told the committee. A zoonotic virus is one that jumps from an animal species to humans.
“The other is that it somehow came out of this National Institute of Virology lab in Wuhan,” he continued. “This is not in some dark part of the web driven by conspiracies. These are reputable people raising very real questions.”
‘Far-fetched ideas’
Liberal MP Peter Fragiskatos accused Chong of spreading disinformation.
“Mr. Chong is proceeding to connect dots here that, you know, he is borrowing from some of the wildest theories on Facebook and other social media to make a point here that is irrelevant to this committee,” he said.
Oliphant said he agrees the documents should be released but called Chong’s comments irresponsible.
“What I am disagreeing with is far-fetched ideas that even hint at some association that makes no sense. And that somehow there is something embedded in these documents that’s going to solve the world’s question about where the coronavirus COVID-19 came from,” Oliphant said.
“That’s bad rhetoric. I think it’s misinformation. I think it’s drawing associations that should not be drawn together at a committee of Parliament. And I think it just cedes the oddest ideas in other people’s heads.”
The National Microbiology Lab in Winnipeg is Canada’s only Level-Four lab, capable of working with the world’s deadliest pathogens. (Trevor Lyons/CBC)
In interview Tuesday with CBC News, Chong clarified and backtracked slightly, saying he was not associating Canada’s lab with the origins of the coronavirus pandemic. He said he merely questioned Canada’s role in training and equipping the lab in Wuhan to get Level-4 certification.
“If it turns out that the Wuhan Institute of Virology is the source of the coronavirus that started this global pandemic, then we need a lot more oversight of the National Microbiology Lab in Winnipeg and the role it played in helping build capacity,” Chong said.
No connections, PHAC says
The RCMP and PHAC have consistently denied any connections between the COVID-19 pandemic and the virus shipments. There is no evidence linking the shipment to the spread of the coronavirus. Ebola is a filovirus and Henipah is a paramyxovirus — the Winnipeg lab sent no coronavirus samples to Wuhan, PHAC said.
“They are not, in fact, at all related and would not have been used or relevant to SARS-CoV-2,” the lab’s scientific director-general, Dr. Guillaume Poliquin, told the committee Monday.
At the conclusion of the meeting, members of the committee passed a motion demanding that unredacted copies of all PHAC records on the matter be turned over to the House of Commons law clerk for review within 10 days.
The committee would then meet in secret to determine what could be released publicly.
The committee also voted to send the matter to the House of Commons if PHAC refuses to produce the documents. Parliament would then be asked to demand disclosure.
My Comment: The secrecy and intransigence in releasing information about details and the manner of treatment of fellow researcher of extra-national origin suggests the Winnipeg lab is a Military Lab and is possibly covertly contracting to the US DOD at the Pentagon. If it were pure science for global public health there would be full and open sharing of scientific data and samples. It wreaks of a probable role for Canada in Biological weapons proliferation.
Expose’ on security breeches were enabled by the Winnipeg Labs collusion with the People’s Liberation Army Biowarfare Agencies.
The Problem is that Vaccines Developed by Canada with dual civilian use military use potential if gained by China means those pathogens cannot be used against China because it confers protection on them. This would compromise offensive use of those pathogens by biowarfare partners in America against China. If they were being developed for international medical public health use their production methodology would be published in peer reviewed medical journals like Nature Medicine or Virology. The scandal exposes the Winnipeg lab as a Partner agency in global biowarfare. ex:
Wuhan Institute of Virology Shao Cao Admission Wuhan Lab Participated in the Search for Best ACE2 Adherent Spike for Weaponization
PERPETRATORS OF THIS HEINOUS CRIME AGAINST HUMANITY
My Summary
The covid-19 virus was designed to harm the immune system by attacking the mitochondrial contribution and the AIDS fragment was included to further attack the immune system. The SV40 fragment found by Japanese investigators is a cancer promoter and specifically can produce several cancers including the same one as asbestos. Loss of the mitochondria increases reactive oxygen and lipid peroxide the same as antibiotics and common pesticides. These are mutagens that can initiate many changes including but not limited to increasing the risk of cancer while loss of oxidative phosphorylation will increase aerobic glycolysis, the favorite respiration of cancer while also damaging the cardiovascular system because the heart is loaded with and mitochondria and needs them as an ATP energy source. You also lose short chain fatty acids which damages the immune system. Mitochondrial genes sustain the immune system and that contribution is diminished by their damage or loss. Data from a number of countries showed that deaths increased significantly after vaccinations. The mRNA experimental drugs are not a vaccine. They neither prevent infection or stop its spread. They don’t work because this virus mutates faster than we can make vaccines. This virus is a population reduction biowarfare agent designed to kill people and the vaccine is part of that mission. Administration of antibiotics to those sick with it may hasten their death. Please see: https://www.researchgate.net/publication/346505752_Antibiotic_induced_changes_to_mitochondria_result_in_potential_contributions_to_carcinogenesis_heart_pathologies_other_medical_conditions_and_ecosystem_risks
See my findings on mitochondria important in considering future side effects.
The Chief Architects of this Depravity
Obama, Biden, Hillary, Many others.
CBC Story on Manitoba Lvl IV Lab Suggest Canada Researching Bioweapons. Is this under contract to US DOD?
These Biological Weapons Revelations Changes Everything
These Revelations Change the Direction and Purpose of the Phony Proxy War from Protection of Sovereignty to Protection of Global Biological War Infrastructure and Perpetrators to Arresting them for Crimes against Humanity and Contributing to Ecocide for Trial at Nuremberg II.
HOW THEY DID IT: They used a particular bug (Coronavirus) that was previously relatively benign and nonpathogenic and modified it through the use of gene editing techniques to make the bug (Covid-19) virulent, pathogenic, dangerous and then released that bug (Covid) in key sites.… Show mor
THEY RELEASED COVID-19: U.S. Patents show CDC ownership of Coronavirus. Both China and the U.S. involved in creating SARS-CoV-2. Bill Gates and CCP appoints criminal Tedros of WHO. The DOD, FDA, CIA, NIH, Fauci, Baric, Daszak, Rockefeller, Rothschilds are all involved in these Crimes.
Bill Gates and the Rockefeller foundation paid Google, Facebook, Politico, Wikipedia, Fact Checkers in order to censor and control all the information. The CIA has been using Operation Mockingbird for years and has over 3,000 agents implanted in Mainstream Media to control the population. Event 201 was sponsored by Bill Gates, the Johns Hopkins Center for Health Security (CIA) and the World Economic Forum to enforce a worldwide Pandemic response 5 months before the WHO fraudulently declared a global pandemic.
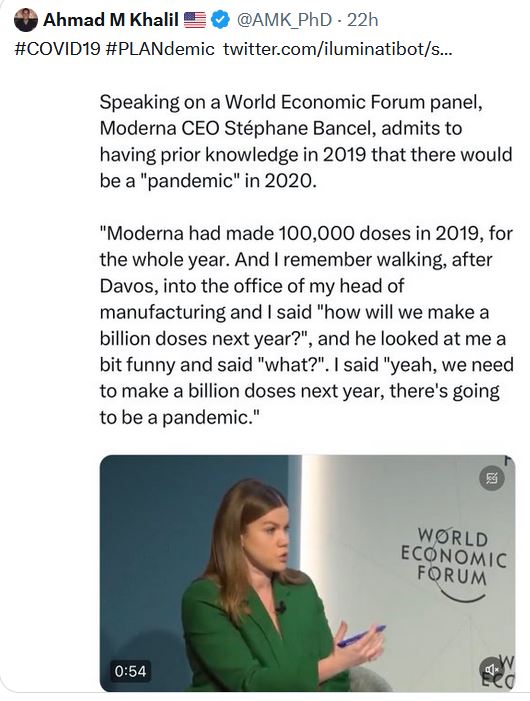
It was a planned coordinated criminal effort worldwide. In January 2017 Anthony Fauci said there will be a surprise virus outbreak before the end of 2020. Bill Gates in 2015 talked of a future pandemic and lied in April 2020 when he said they did not simulate or practice for a pandemic.
Klaus Schwab in his book Covid-19 The Great Reset shows Covid was the Trojan Horse to Reset the World according to the UN 2030 Agenda. Build Back Better slogan is a criminal coordinated effort to remove human rights and institute a one world government.
Bill Gates and the Rockefeller foundation bribes the WHO, NIH, NIAID, CDC, FDA, Medical Schools and Journals to control the health industry and public health policy.
WHO Chief Tedros involved in genocide killing and torture in Ethiopia. Tedros is a known member of the communist party. He is Beijing’s and Gates puppet. As a Health Minister he was accused of covering up three Cholera Epidemics and committing crimes against humanity. CCP and Bill Gates helped put Tedros in charge of the WHO. John D. Rockefeller over 100 years ago seized the U.S. Media and took control over public health using toxic petroleum based drugs for profit and controlled the American Medical Association blacklisting and expelling any doctors who practiced natural medicine. Rockefeller’s poison injections and medicines started causing cancer in early years and to cover it up formed the American Cancer Society. Medical error is the 3rd leading cause of death in America.
Bill Gates used India and Africa as guinea pigs for pharmaceutical companies to make a financial killing while killing a lot of people in the process including killing innocent children and babies with vaccines. Bill Gates controls GAVI The Vaccine Alliance to vaccinate the world with his poisons.
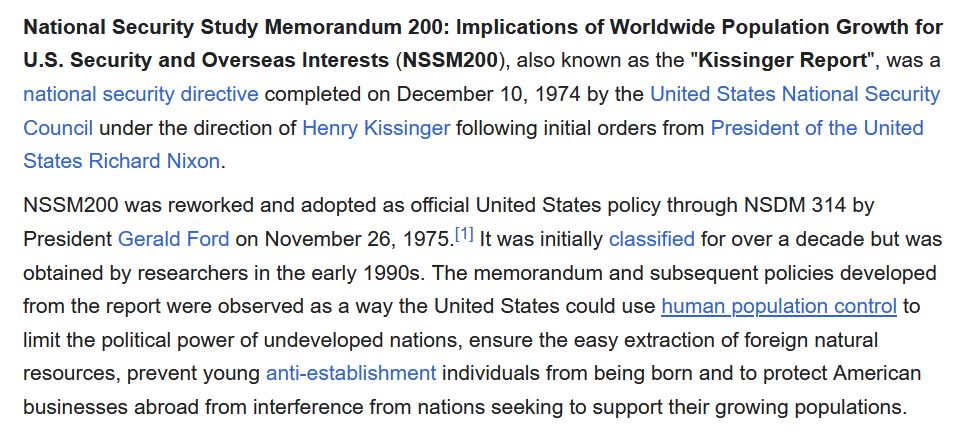
National Security Study Memorandum NSSM 200 Implications of Worldwide Population Growth For U.S. Security and Overseas Interests December 10, 1974 (THE KISSINGER REPORT) shows the intention of governments to reduce the population. Bill Gates is one of the key funders in the Stratosphere experiment to block out the sun for Climate Change by releasing poisons in the air. Environmental Scientist call it global genocide experiment.
Gates has invested over one billion dollars in the Earth Now Global Surveillance project to launch hundreds of satellites to monitor people everywhere 24/7 a day. In partnership with MIT Bill Gates has developed a new technology that allows vaccines to be injected under your skin along with your medical records. Bill Gates Gates funded genetically modified mosquitoes released in the USA to allow human immunization by means of mosquito bites “Flying Syringes.” Gates had business dealings and a relationship with Jeffrey Epstein, a convicted child sex criminal. Why would he choose to partner with the world’s most notorious pedophile? Gates is the top financial donor of the WHO and CDC. No one person has more power than Gates to influence and control the health and medical freedom of all people. Bill Gates and all mRNA Vaccines must be stopped. This is a global genocide experiment and a takeover of humanity.
THEY RELEASED COVID-19: U.S. Patents show CDC ownership of Coronavirus. Both China and the U.S. involved in creating SARS-CoV-2. Bill Gates and CCP appoints criminal Tedros of WHO. The DOD, FDA, CIA, NIH, Fauci, Baric, Daszak, Rockefeller, Rothschilds are pic.twitter.com/POFAcPf7Yo…